Do you NEED to experience those awful menstrual cramps? No. You might not be able to eliminate them entirely, but they can be reduced through diet and nutrition!
Almost every female I know has a story about terrible cramps and how they missed an important event or had to miss a game or had to almost overdose on pain meds due to menstrual cramps. Don’t let this be you!
TLDR: Eat real food (fruits, vegetables, whole grains, beans, nuts and seeds, herbs and spices, fatty fish), exercise most days, get enough sleep, and stay hydrated. Don’t smoke and limit junk food and added sugar. Vitamin D and omega-3 fatty acid supplementation might be useful.
How Big of a Problem are Menstrual Cramps?
Menstrual cramps, or period cramps, are officially known as “primary dysmenorrhea,” or lower abdominal pain that occurs before/during the menstrual cycle but isn’t caused by other medical issues.1 Dysmenorrhea is a Greek phrase for “painful monthly bleeding.”
Secondary dysmenorrhea is caused by those other medical issues in or around the uterus. Talk to your doctor about those!
Main treatments for primary dysmenorrhea are OTC painkillers, birth control pills, and lifestyle changes. If these don’t help, see point #2, above, and get help!
Menstrual cramps start anywhere from two days before to the start of menstrual flow and last for up to three days.2 They affect almost every person capable of having a period (people with a functional uterus, between menarche and menopause). Depending on the study, cramps impact somewhere between 16% to 95% of women during their reproductive years.1.2 29% – 40% of those experiencing those cramps rate them as “severe.”
Lifespan Changes
Menstrual cramps change over the lifespan. Rates are very low for the first 6-24 months after menarche, then skyrocket through adolescence and early adulthood.1,2 Adolescents and younger women seem to have more severe cramps, up to 70-90%. They taper off through the next few decades until they’re much less severe before menopause. They’re also worse in women who have NOT had kids and those who HAVE had a Caesarean section.1,3
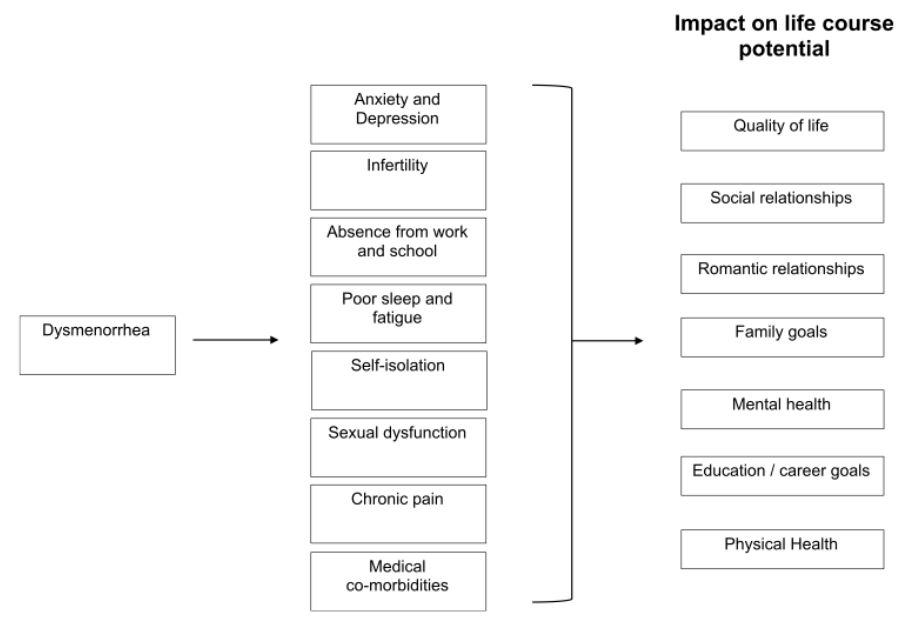
Four Types of Physical and Emotional Effects
Side effects of menstrual cramps span the body and appear either before or during menstruation.
- Systemic: Headache, body/joint pains, lethargy, fatigue, sleep disorders, tender breasts, swollen legs, low back pain, dizziness, water retention, weight gain
- Gastrointestinal: appetite changes, nausea, indigestion, vomiting, bloating
- Elimination-related: constipation, diarrhea (or both together, yay!), frequent urination, hyper perspiration (extreme sweating)
- Psychological: Anxiety, depression, nervousness, irritability, mood swings
Quality of Life Suffers
Quality of life also suffers, with up to 1/3 of women claiming a drop in life satisfaction and performance. Absenteeism rises, as almost 1/8 women skip work or school during this time.1
The US loses around 140 million work hours/year to menstrual cramps, so there’s an economic impact too!1 US residents that menstruate lose an average of 6 days’ work/year.5 A Dutch study reported an average of 9 days’ work lost/year.6
In a Hungarian study, one third of women missed school or work at least once/cycle.7 The women with severe muscle cramps were willing to pay on average €1127 ($1240 in 2023 exchange rates) to eliminate them entirely, while women who had mild issues were willing to pay only €142 ($156).
In a Japanese study, women with cramps spent 2.2 times as much on health care compared to women without cramps for an extra eight physician visits per year and medication.8
Physiological Causes of Menstrual Cramps
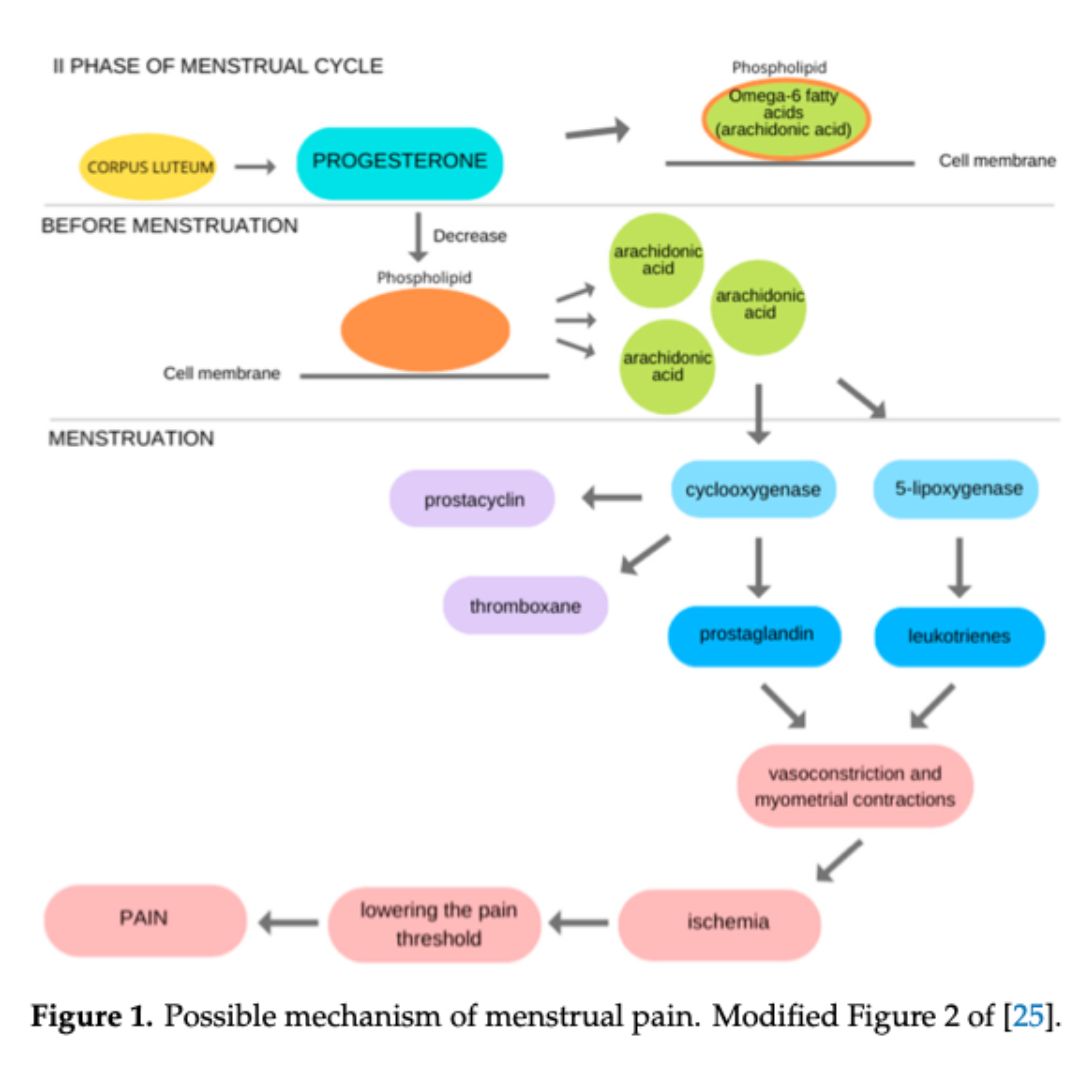
Inflammation
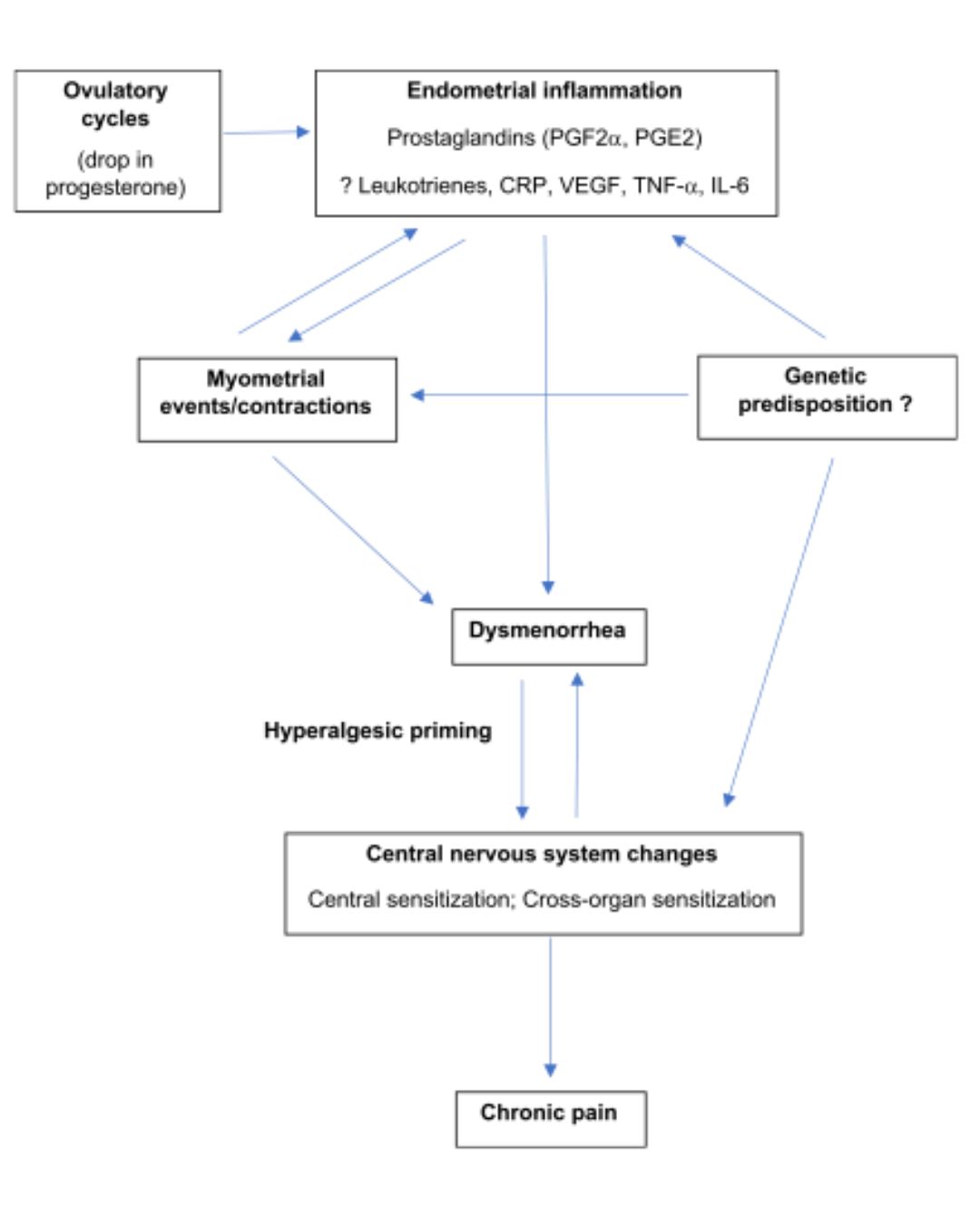
Progesterone rises in the second half of the menstrual cycle, the luteal phase. It allows the uterus to build a lining in case there’s a fertilized egg that needs to implant somewhere. No egg, no implantation? Progesterone drops and prostaglandins rise. Prostaglandin F2alpha (PGF-2a) increases uterine muscle contractions, allowing the uterus to shed the uterine lining built up during the luteal phase of the menstrual cycle.2
Prostaglandins are a downstream product of a dietary omega-6 essential fatty acid, linoleic acid (18:2n6c), which is modified into arachidonic acid (20:4n6). Either of those or intermediate fatty acids consumed in the diet become part of our cell membranes.
Women with more cramps have higher levels of prostaglandins than women with few/no cramps.
There might be a genetic influence on menstrual cramps. The mu-opioid receptor (OPRM1) gene has two versions. The A version regulates pain; the G version impedes this regulation.11 This single nucleotide polymorphism (A118G) leads to less OPRM1, more pain and more pain-relieving medication use.
Untreated menstrual cramps can lead to hyperalgesic priming, or enhanced pain sensitivity in the pelvic area.9 There may be racial differences, with less effect in Asian populations.12It pays to treat this pain early and often, as well as consistently across the lifespan, for less pain overall!
Nutrition Quality Makes A Difference in Menstrual Cramps
Medicinal plants (AKA whole foods, herbs and spices) have a variety of low-quality studies.13 Ginger is a common choice; it has benefits beyond nausea and indigestion!14These plants contain a wide variety of useful plant chemicals that function as anti-oxidant and anti-inflammatory compounds as well as fiber, vitamins and minerals. Eat more of these to feel better. It’s almost like being well-nourished helps… Relatedly, eating <3 servings of fruit/week leads to more cramping.15
Omega-3 Fatty Acids
How are they made in the body?
Omega-3 Fatty acids use the same enzymes as Omega-6 fatty acids to get from food components to useful compounds in cells. We must get enough omega-3s to balance out the omega-6 fatty acids discussed above. While the omega-6 fatty acids are primarily precursors to inflammation, omega-3 fatty acids primarily work to resolve or reduce that inflammation.16
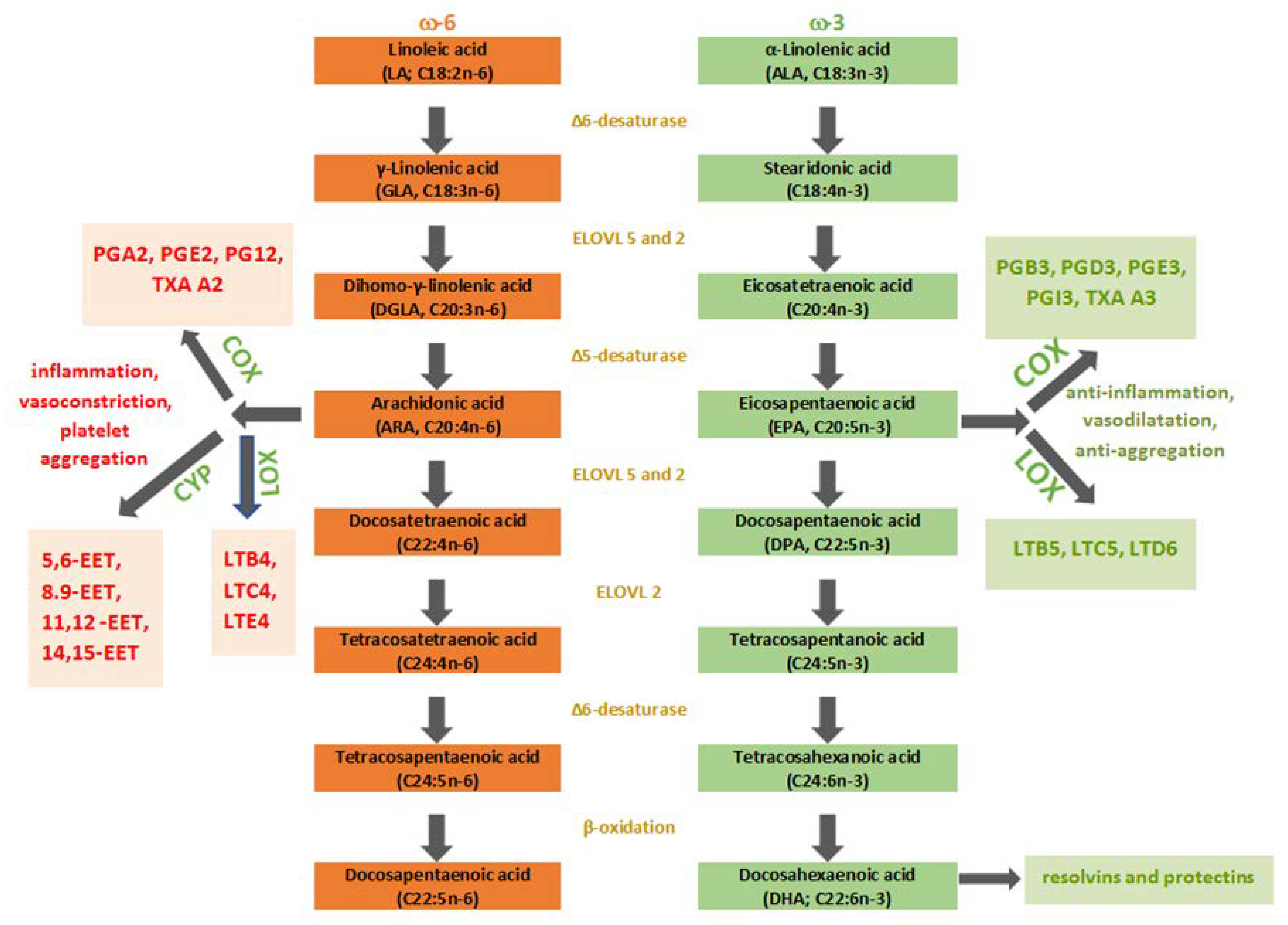
Omega-3 Fatty Acids Reduce Cramping by Balancing Omega-6 Fatty Acids
Fish intake reduced menstrual cramps in a Japanese study based on the theory that fish are high in omega-3 fatty acids.17 Not all fish are high in omega-3 fatty acids! However, compared to women in the study that never ate fish, having at least 4 servings of fish/week reduced moderate/severe menstrual cramp pain by half. HALF!
An Iranian study that provided vitamin E, omega-3 fatty acids (a comparatively low dose of 300 mg combined EPA and DHA), both or neither indicated that both vitamin D and omega-3 fatty acids reduced cramping, but the combination had the most powerful effects.18 Pain scores dropped from ~7 to ~4 on a scale of 1-10 with the combo.
Sources of omega-3s: fish, some nuts and seeds, supplements.19 Our requirement is somewhere between 1 and 1.6 g/day, depending on age and sex. If taking supplements, be sure to look at two things. 1) the number of capsules to consume daily (it’s probably not one!) 2) The amount of EPA/DHA in the capsules. Get the supplements with a high percentage of EPA/DHA in the fish oil. We don’t care about the rest of the fish oil, just those two key omega-3 fatty acids. Buy the 800 mg EPA/DHA per 1000 mg fish oil, NOT the 25 mg EPA/DHA per 1000 mg fish oil. Find info on safe, banned-substance-free supplements here.
Vitamin D
Vitamin D studies are widely varied, but indicate a possible effect of HIGH dose vitamin D. This makes sense, as one of vitamin D’s many roles is regulating inflammation.20 Most studies used 50,000 IU weekly or a couple of times/day going into the bleeding phase of the cycle to get an effect.21,22 The RDA for Vitamin D in the US is somewhere between 400 IU and 800 IU, depending on age and sex.20 50,000 IU would typically be a clinical solution to vitamin D deficiency. It’s probably not a practical solution for most people. But you should make sure that you’re sufficient, even if that means supplementing all or most of the year. Read more about vitamin D here!
Vitamin A
Vitamin A status might also contribute to overall antioxidant status and menstrual cramps. Bahrami showed a significantly lower vitamin A status in women with cramps than those without (and an even greater difference in those with severe PMS!).23
Alcohol
Alcohol has a small protective effect, but since it’s pretty much negative for everything else including general health and sports performance, think carefully about this before trying it.24 AKA: Don’t drink.
Other Negatives: dehydration, sugar, caffeine
Other things that have a negative effect include dehydration, high sugar intake, and drinking caffeinated beverages.15
Lifestyle Factors Beyond Nutrition That Affect Menstrual Cramps
Exercise
Great news! Exercise helps, both with duration and intensity of pain.25,26 On a 10-point scale, regular exercise reduces pain by about 2.5 points. Type doesn’t seem to matter so much as dose: 45-60 minutes at least three times per week.
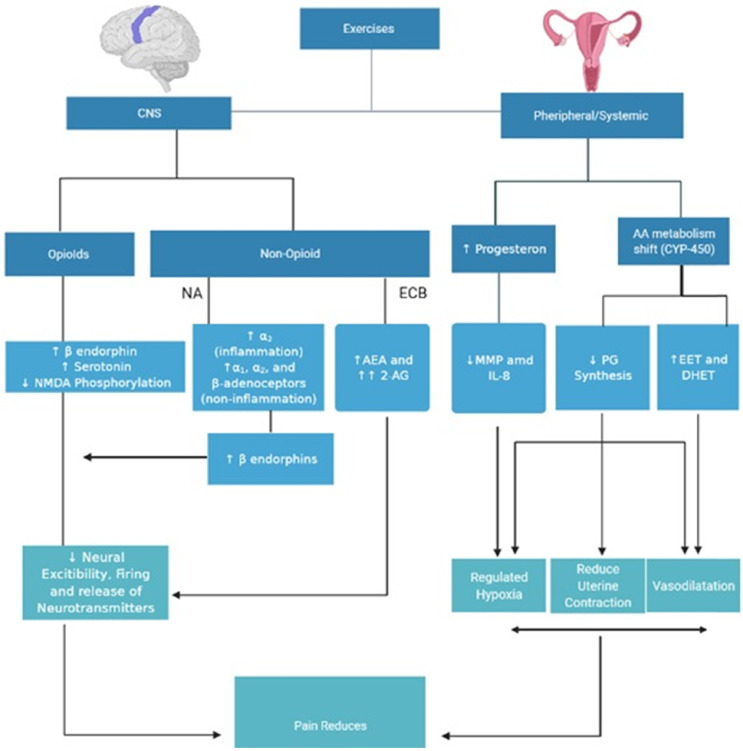
Pain is reduced via several pathways. Note the reduction of “PG synthesis” on the right side: fewer prostaglandins! Also endorphins are produced through the exercise.
Not getting enough sleep (<7 hours/night) increased cramping.15 Getting exercise improves sleep quality in case you can’t get enough sleep.28
Smoking absolutely makes menstrual cramps worse!24 It doubles the risk of pain for those smoking about a pack a day and almost triples the risk of pain for those who have smoked longer than 10 years.
To Do:
- Eat real food. This means fish, water, fruits, vegetables, whole grains, beans, nuts, seeds, and herbs and spices.
- Skip the processed foods 80% of the time unless you are actively training or recovering from training. If it’s post-season or you have a major competition or competition period coming up, make it 90% of the time.
- Supplement if you need to. Please remember to choose supplements with third party testing!
Need Help with Applying This Content To YOU?
If you need help figuring out how to include the foods above into your training or competition meal plans, contact Dr. Schubert!
Check out a blog on the theoretical changes in food intake needed across the different menstrual cycle phases independent of menstrual cramps. Craving chocolate at that time of the month? Here are some ways to take advantage of those cravings. Saw my comment about caffeine making cramps worse and need to know more? Here’s that article!
References
- Nagy H, Khan MAB. Dysmenorrhea. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www-ncbi-nlm-nih-gov.libweb.ben.edu/books/NBK560834/
- Itani R, Soubra L, Karout S, Rahme D, Karout L, Khojah HMJ. Primary Dysmenorrhea: Pathophysiology, Diagnosis, and Treatment Updates. Korean J Fam Med. 2022;43(2):101-108. doi:10.4082/kjfm.21.0103
- Santos LBD, Barbosa IR, Dantas THM, et al. Prevalence of primary dysmenorrhea and associated factors in adult women. Rev Assoc Med Bras (1992). 2022;68(1):31-36. doi:10.1590/1806-9282.20210341
- Lete I, Häusler G, Pintiaux A, et al. The inconvenience due to women’s monthly bleeding (ISY) survey: a study of premenstrual symptoms among 5728 women in Europe. Eur J Contracept Reprod Health Care. 2017;22(5):354-359. doi:10.1080/13625187.2017.1400001
- Ponzo S, Wickham A, Bamford R, et al. Menstrual cycle-associated symptoms and workplace productivity in US employees: A cross-sectional survey of users of the Flo mobile phone app. Digit Health. 2022;8:20552076221145852. Published 2022 Dec 15. doi:10.1177/20552076221145852
- Schoep ME, Adang EMM, Maas JWM, De Bie B, Aarts JWM, Nieboer TE. Productivity loss due to menstruation-related symptoms: a nationwide cross-sectional survey among 32 748 women. BMJ Open. 2019;9(6):e026186. Published 2019 Jun 27. doi:10.1136/bmjopen-2018-026186
- Rencz F, Péntek M, Stalmeier PFM, et al. Bleeding out the quality-adjusted life years: evaluating the burden of primary dysmenorrhea using time trade-off and willingness-to-pay methods. Pain. 2017;158(11):2259-2267. doi:10.1097/j.pain.0000000000001028
- Akiyama S, Tanaka E, Cristeau O, Onishi Y, Osuga Y. Evaluation of the treatment patterns and economic burden of dysmenorrhea in Japanese women, using a claims database. Clinicoecon Outcomes Res. 2017;9:295-306. Published 2017 May 22. doi:10.2147/CEOR.S127760
- MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O. Disease Burden of Dysmenorrhea: Impact on Life Course Potential. Int J Womens Health. 2023;15:499-509. Published 2023 Apr 3. doi:10.2147/IJWH.S380006
- Barcikowska Z, Rajkowska-Labon E, Grzybowska ME, Hansdorfer-Korzon R, Zorena K. Inflammatory Markers in Dysmenorrhea and Therapeutic Options. Int J Environ Res Public Health. 2020;17(4):1191. Published 2020 Feb 13. doi:10.3390/ijerph17041191
- Hsu PS, Cheng CM, Chao HT, et al. OPRM1A118G polymorphism modulating motor pathway for pain adaptability in women with primary dysmenorrhea. Front Neurosci. 2023;17:1179851. Published 2023 Jun 12. doi:10.3389/fnins.2023.1179851
- Lee LC, Chen YY, Li WC, et al. Adaptive neuroplasticity in the default mode network contributing to absence of central sensitization in primary dysmenorrhea. Front Neurosci. 2023;17:1094988. Published 2023 Feb 9. doi:10.3389/fnins.2023.1094988
- Pellow J, Nienhuis C. Medicinal plants for primary dysmenorrhoea: A systematic review. Complement Ther Med. 2018;37:13-26. doi:10.1016/j.ctim.2018.01.001
- Crichton M, Davidson AR, Innerarity C, et al. Orally consumed ginger and human health: an umbrella review. Am J Clin Nutr. 2022;115(6):1511-1527. doi:10.1093/ajcn/nqac035
- Al-Husban N, Odeh O, Dabit T, Masadeh A. The Influence of Lifestyle Variables on Primary Dysmenorrhea: A Cross-Sectional Study. Int J Womens Health. 2022;14:545-553. Published 2022 Apr 13. doi:10.2147/IJWH.S338651
- Balić A, Vlašić D, Žužul K, Marinović B, Bukvić Mokos Z. Omega-3 Versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. International Journal of Molecular Sciences. 2020; 21(3):741. https://doi.org/10.3390/ijms21030741
- Yokoyama E, Takeda T, Watanabe Z, et al. Association of fish intake with menstrual pain: A cross-sectional study of the Japan Environment and Children’s Study. PLoS One. 2022;17(7):e0269042. Published 2022 Jul 21. doi:10.1371/journal.pone.0269042
- Sadeghi N, Paknezhad F, Rashidi Nooshabadi M, Kavianpour M, Jafari Rad S, Khadem Haghighian H. Vitamin E and fish oil, separately or in combination, on treatment of primary dysmenorrhea: a double-blind, randomized clinical trial. Gynecol Endocrinol. 2018;34(9):804-808. doi:10.1080/09513590.2018.1450377
- National Institutes of Health, Office of Dietary Supplements. Omega-3 Fatty Acids: Fact Sheet for Consumers. Updated July 18, 2022. Accessed August 12, 2023. https://ods.od.nih.gov/factsheets/Omega3FattyAcids-Consumer/.
- National Institutes of Health, Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. Updated August 12, 2022. Accessed August 14, 2023. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/.
- Amzajerdi A, Keshavarz M, Ghorbali E, Pezaro S, Sarvi F. The effect of vitamin D on the severity of dysmenorrhea and menstrual blood loss: a randomized clinical trial. BMC Womens Health. 2023;23(1):138. Published 2023 Mar 27. doi:10.1186/s12905-023-02284-5
- Chen YC, Chiang YF, Lin YJ, et al. Effect of Vitamin D Supplementation on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients. 2023;15(13):2830. Published 2023 Jun 21. doi:10.3390/nu15132830
- Bahrami A, Bahrami-Taghanaki H, Khorasanchi Z, et al. Menstrual problems in adolescence: relationship to serum vitamins A and E, and systemic inflammation. Arch Gynecol Obstet. 2020;301(1):189-197. doi:10.1007/s00404-019-05343-1
- Parazzini F, Tozzi L, Mezzopane R, Luchini L, Marchini M, Fedele L. Cigarette smoking, alcohol consumption, and risk of primary dysmenorrhea. Epidemiology. 1994;5(4):469-472. doi:10.1097/00001648-199407000-00016
- Carroquino-Garcia P, Jiménez-Rejano JJ, Medrano-Sanchez E, de la Casa-Almeida M, Diaz-Mohedo E, Suarez-Serrano C. Therapeutic Exercise in the Treatment of Primary Dysmenorrhea: A Systematic Review and Meta-Analysis. Phys Ther. 2019;99(10):1371-1380. doi:10.1093/ptj/pzz101
- Armour M, Ee CC, Naidoo D, et al. Exercise for dysmenorrhoea. Cochrane Database Syst Rev. 2019;9(9):CD004142. Published 2019 Sep 20. doi:10.1002/14651858.CD004142.pub4
- Jaleel G, Shaphe MA, Khan AR, et al. Effect of Exercises on Central and Endocrine System for Pain Modulation in Primary Dysmenorrhea. J Lifestyle Med. 2022;12(1):15-25. doi:10.15280/jlm.2022.12.1.15
- Kirmizigil B, Demiralp C. Effectiveness of functional exercises on pain and sleep quality in patients with primary dysmenorrhea: a randomized clinical trial. Arch Gynecol Obstet. 2020;302(1):153-163. doi:10.1007/s00404-020-05579-2